
Subscribe to our newsletter and get your FREE guide,
L5-S1 Symptoms Tracker.
Conditions affecting the L5-S1 spinal motion segment are usually treated with nonsurgical methods. If the lower back and/or leg symptoms worsen or do not improve despite these treatments, or in case of certain medical emergencies, such as tumors or cauda equina syndrome, surgery may be recommended.
In This Article:
Nonsurgical Treatments for L5-S1
Treatment of L5-S1 usually begins with:
Medication
Over-the-counter (OTC) medications, such as non-steroidal anti-inflammatory drugs (NSAIDs) are usually tried first for pain stemming from L5-S1. For more severe pain, prescription medication, such as opioids, tramadol, and/or corticosteroids may be used.
Physical therapy
Specific exercises and physical therapies can be designed to target pain stemming from L5-S1. These therapies help stabilize the back and keep the muscles and joints well-conditioned for long-term relief, while also providing a healing environment for the tissues in the lower back.
See Physical Therapy for Low Back Pain Relief
Chiropractic manipulation

Chiropractic adjustments may help relieve lumbar pain.
Manipulation of the lumbar spine through chiropractic adjustment may help relieve pain stemming from L5-S1.
Self-care
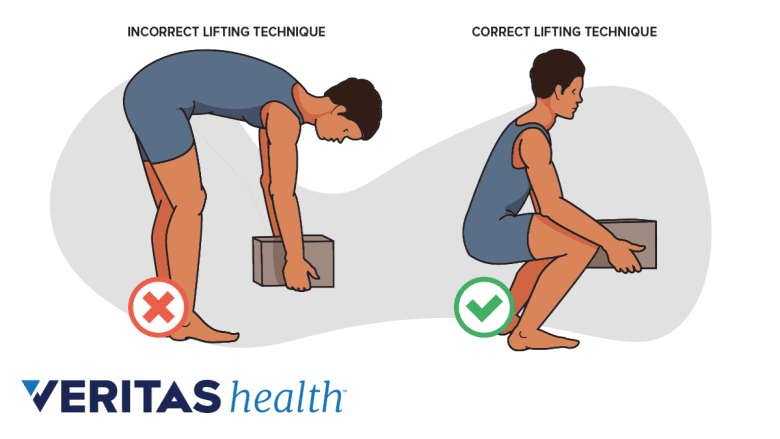
Using a supported posture while bending and lifting helps protect the spinal structures.
Mild to moderate pain may be treated with heat and ice at home. For sciatica pain, it is advised to stay active and continue daily activities as tolerated. While bed rest may provide temporary relief from symptoms, it usually does not aid in faster or long-term recovery for sciatica.
Following an exercise routine, quitting smoking, and reducing weight in overweight individuals can help lower the risk of problems stemming from L5-S1.
advertisement
Injection Treatments for L5-S1
Injections may be considered for pain relief after nonsurgical methods are tried for several weeks and before surgery is considered.
Common injection treatments for L5-S1 include:
Lumbar epidural steroid injections
Steroids injected directly into the spinal epidural space can help decrease inflammation and reduce the sensitivity of nerve fibers to pain, generating fewer pain signals. These injections are more effective in treating the inflammatory causes of pain, such as pain from herniated disc fragments, and are typically less effective for compressive causes of pain.
See Lumbar Epidural Steroid Injections for Low Back Pain and Sciatica
Radiofrequency ablation
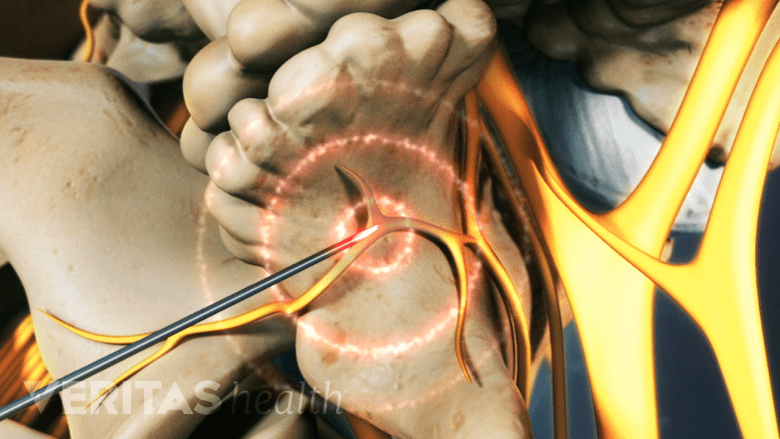
Targeted application of heat to a nerve can be used to interrupt its pain pathway.
Radiofrequency ablation may be used to treat pain stemming from the L5-S1 facet joints. A part of the pain-transmitting nerve is heated with a radiofrequency needle to create a heat lesion. This resulting lesion prevents the nerve from sending pain signals to the brain.
While performing injection treatments, fluoroscopic (x-ray) guidance is usually used for correct needle placement. Fluoroscopic guidance and contrast dye help improve diagnostic accuracy and decreases procedural risks.
Injections may also be used diagnostically as a selective nerve block to confirm the nerve root as the cause of the leg pain and may be helpful as a diagnostic aid prior to surgery.
Surgical Treatments for L5-S1
When the neurological deficits, such as numbness and/or weakness continue to worsen despite several weeks of nonsurgical treatments, surgery may be recommended. Surgery is considered when a structural condition that is known to be responsive to surgical treatment is present.
Surgeries to relieve compression of a nerve root and/or the cauda equina include:
- Microdiscectomy: A small part of the disc material near the nerve root is taken out. A portion of the bone adjacent to the nerve root may also be trimmed to relieve compression.
- Laminectomy: A part or all of the lamina (area of bone at the back of the vertebra) is removed in order to provide more room for the cauda equina.
- Foraminotomy: The opening for the spinal nerve root (intervertebral foramen) is enlarged by trimming bony overgrowth, relieving compression.
- Facetectomy: The facet joints are trimmed to relieve compression of nerve roots.
- Lumbar interbody fusion: A degenerated disc is removed and L5-S1 vertebrae are fused together with implants or bone grafts. While performing a fusion surgery, the spinal fixation of the S1 segment usually presents a greater risk of failure (pseudarthrosis) compared to L5. To avoid this complication, the addition of an interbody support (device that holds the vertebrae together) is typically recommended to increase the likelihood of a successful fusion at L5-S1.
Watch L5-S1 Anterior Lumbar Interbody Fusion Surgery Animation
Surgeons may perform more than one procedure at a time. For example, a laminoforaminotomy is when a laminectomy procedure is done along with a foraminotomy. While minimally invasive techniques are used for these surgeries, open surgeries may be performed in some cases.
advertisement
Some patients who do not have progressive neurological changes may not respond to nonsurgical care. They may also not be good candidates for surgery due to other medical problems or drug addiction, to name a few.
A small risk of serious complications, such as infection, nerve injury, excessive bleeding, or severe allergic reactions are possible with spine surgeries. Before deciding to have surgery, it is important to discuss the risks and alternatives to surgery with a surgeon. It is also important to understand the possible complications if surgery is not performed.

advertisement
Editor’s Top Picks
- Epidural Steroid Injections for Back Pain and Leg Pain Video
- Understanding L5-S1 Spinal Fusion Animation
- Sciatica Treatment Video
- Microdiscectomy Spine Surgery: Risks, Complications, and Success Rates
- Lumbar Herniated Disc Treatment Video
- Lumbar Laminectomy Surgery for Spinal Stenosis (Open Decompression)