
The L4 and L5 are the two lowest vertebrae of the lumbar spine. Together with the intervertebral disc, joints, nerves, and soft tissues, the L4-L5 spinal motion segment provides a variety of functions, including supporting the upper body and allowing trunk motion in multiple directions.1Waldman SD. Functional Anatomy of the Lumbar Spine. In: Pain Review. Elsevier; 2009:65-66. doi:10.1016/b978-1-4160-5893-9.00029-0
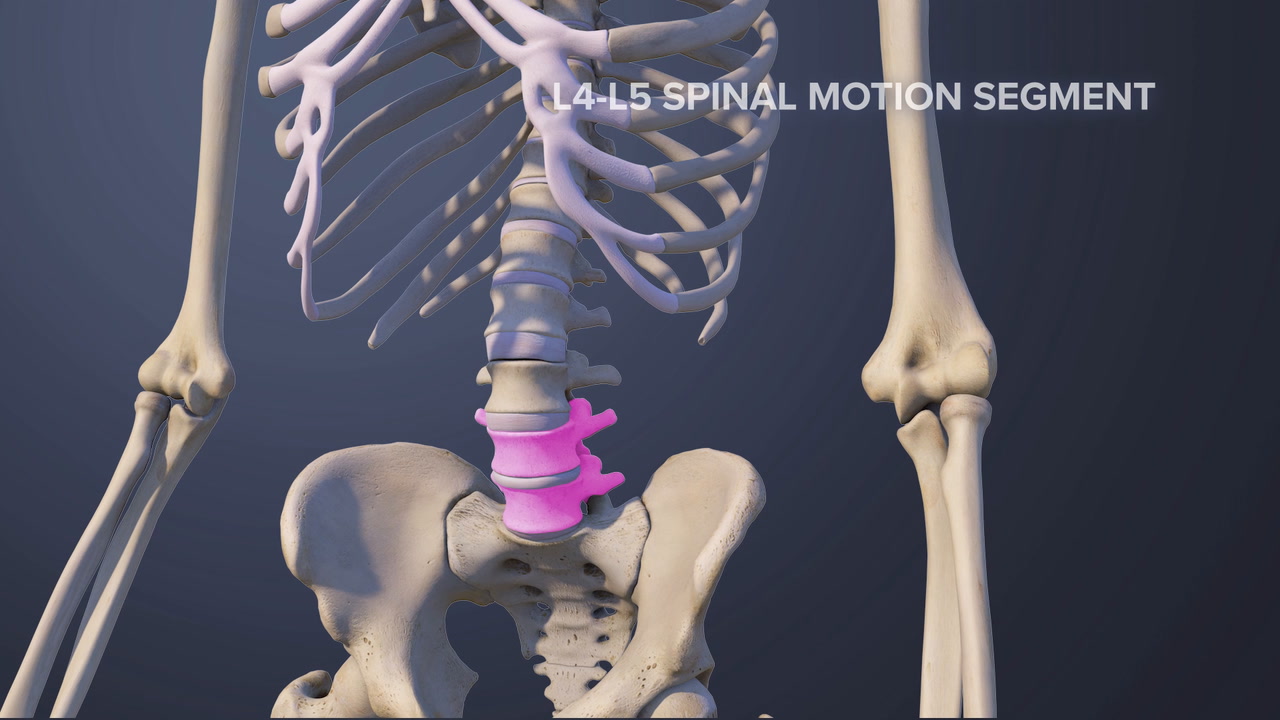
Due to its heavy load-bearing function and wide range of flexibility, the L4-L5 motion segment may be more susceptible to developing pain from injury and/or degenerative changes compared to other lumbar segments.2Cramer GD. The Lumbar Region. In: Clinical Anatomy of the Spine, Spinal Cord, and Ans. Elsevier; 2014:246-311. doi:10.1016/b978-0-323-07954-9.00007-4
In This Article:
- All About the L4-L5 Spinal Segment
- L4-L5 Treatment
- Spinal Motion Segment: L4-L5 Animation
Anatomy of the L4-L5 Spinal Motion Segment
The L4-L5 motion segment includes the following structures:
L4 and L5 vertebrae

The L4 and L5 vertebrae are sturdy bone structures that form the base of the lumbar portion of the spine.
Each vertebra consists of a vertebral body in front and a vertebral arch at the back. The vertebral arch has 3 bony protrusions: a prominent spinous process in the middle and two transverse processes on either side. The region between the spinous process and the transverse process is called the lamina. The region between the transverse process and the vertebral body is called the pedicle. The vertebrae are joined by facet joints (zygapophyseal joints), which are covered by articulating cartilage to provide smooth movements between the joint surfaces.
The L4 and L5 vertebral bodies are taller in front than behind. The upper and lower ends of each vertebral body are covered by bony endplates that help resist compressive loads placed on the spine.2Cramer GD. The Lumbar Region. In: Clinical Anatomy of the Spine, Spinal Cord, and Ans. Elsevier; 2014:246-311. doi:10.1016/b978-0-323-07954-9.00007-4
L4-L5 intervertebral disc

The L4-L5 disc protects and structurally supports the vertebrae.
A disc made of a gel-like material (nucleus pulposus) surrounded by a thick fibrous ring (annulus fibrosus) is situated between the vertebral bodies of L4 and L5. This disc provides cushioning and shock-absorbing functions to protect the vertebrae from grinding against each other during spinal movements.
The height of the L4-L5 disc plays an important role in maintaining the lordosis (inward curvature) of the lumbar spine.2Cramer GD. The Lumbar Region. In: Clinical Anatomy of the Spine, Spinal Cord, and Ans. Elsevier; 2014:246-311. doi:10.1016/b978-0-323-07954-9.00007-4
Watch Lumbar Disc Anatomy Animation
L4 spinal nerve
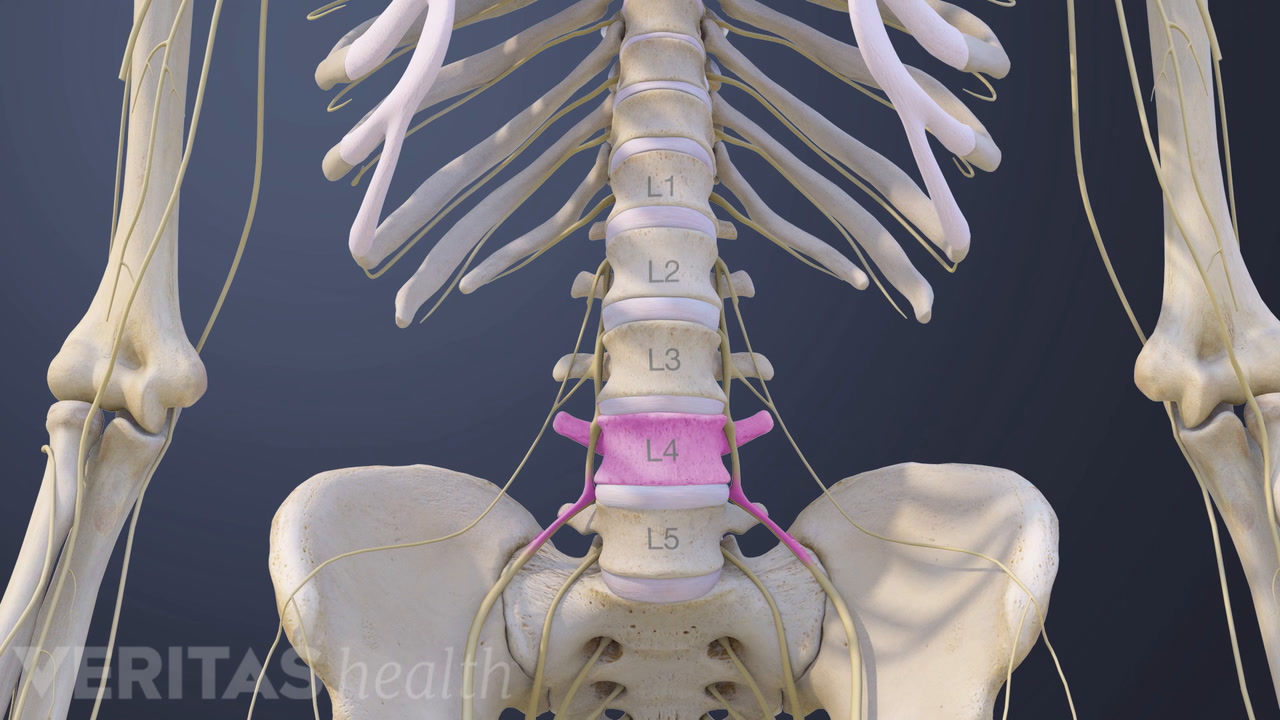
The L4 spinal nerve roots exit the spinal cord through small bony openings (intervertebral foramina) on the left and right sides of the spinal canal. These nerve roots join with other nerves to form bigger nerves that extend down the spine and travel down each leg.
- The L4 dermatome is an area of skin that receives sensations through the L4 spinal nerve and includes parts of the thigh, knee, leg, and foot.
- The L4 myotome is a group of muscles controlled by the L4 spinal nerve and includes parts of several muscles in the back, pelvis, thigh, leg, and foot.3Kayalioglu G. The Spinal Nerves. In: The Spinal Cord. Elsevier; 2009:37-56. doi:10.1016/b978-0-12-374247-6.50008-0
The L4-L5 motion segment provides a bony enclosure for the cauda equina (nerves that continue down from the spinal cord) and other delicate structures.1Waldman SD. Functional Anatomy of the Lumbar Spine. In: Pain Review. Elsevier; 2009:65-66. doi:10.1016/b978-1-4160-5893-9.00029-0
Common Problems at L4-L5
Some of the more common injuries and disorders that may occur at the L4-L5 motion segment include:
Facet joint problems
The high degree of mobility at L4-L5 makes this motion segment prone to facet joint related problems, such as osteoarthritis2Cramer GD. The Lumbar Region. In: Clinical Anatomy of the Spine, Spinal Cord, and Ans. Elsevier; 2014:246-311. doi:10.1016/b978-0-323-07954-9.00007-4, synovial cyst (fluid-filled sac) formation, and instability of the facets.
Disc problems

Due to the high stresses placed on the L4-L5 segment, the disc is prone to degeneration.
The L4-L5 disc is at a high risk of degeneration. This risk may be due to increased loads at the L4-L5 motion segment and decreased movement in the segments below this level. A change in disc height due to degeneration may affect the lordosis of the lumbar spine.2Cramer GD. The Lumbar Region. In: Clinical Anatomy of the Spine, Spinal Cord, and Ans. Elsevier; 2014:246-311. doi:10.1016/b978-0-323-07954-9.00007-4 The disc may also herniate due to degeneration or injury.4Amin RM, Andrade NS, Neuman BJ. Lumbar Disc Herniation. Curr Rev Musculoskelet Med. 2017;10(4):507–516. doi:10.1007/s12178-017-9441-4
See Lumbar Herniated Disc: What You Should Know
Spondylolysis
A fracture of the pars interarticularis (a small segment of bone from the vertebral arch joining the facet joints) can occur at the L4-L5 level due to concentration of compressive loads in this region.2Cramer GD. The Lumbar Region. In: Clinical Anatomy of the Spine, Spinal Cord, and Ans. Elsevier; 2014:246-311. doi:10.1016/b978-0-323-07954-9.00007-4 It can occur on one or both sides. Frequently, the bone does not break, but becomes stressed and this condition is called a pars stress reaction.
Watch Lumbar Spondylolysis Video
Degenerative spondylolisthesis

The angle of the L4-L5 facet joint changes with age, making this level susceptible to spondylolisthesis (forward slippage of L4 on L5) due to degenerative changes in individuals over 60 years of age.2Cramer GD. The Lumbar Region. In: Clinical Anatomy of the Spine, Spinal Cord, and Ans. Elsevier; 2014:246-311. doi:10.1016/b978-0-323-07954-9.00007-4
See Degenerative Spondylolisthesis
Spinal stenosis

Degenerative changes in the bony openings can inflame the nerves that pass through them.
Narrowing (stenosis) of bony openings for nerves due to the presence of bone spurs (abnormal bone growth) or other degenerative changes may cause compression of the nerve roots in the area of stenosis.
External trauma from falls or motor vehicle accidents may cause facet joint dislocation, fracture, and/or damage to the cauda equina at this level. Rarely, tumors and infections may affect the L4-L5 vertebrae and spinal segment.
Common Symptoms and Signs Stemming from L4-L5

Problems in the L4-L5 segment can cause pain in the lower back and legs.
The L4-L5 motion segment may cause referred pain from the joints and/or muscles or radicular symptoms that travel through nerves. Referred pain from L4-L5 usually stays within the lower back and is typically felt as a dull ache. The back may also feel stiff.
Depending on the type and severity of the underlying cause, the L4-L5 motion segment may cause lumbar radicular pain of the L4 and/or L5 spinal nerves, also called sciatica. Common symptoms and signs include:
- Sharp pain, typically felt as a shooting and/or burning feeling that originates in the lower back and travels down the leg in the distribution of a specific nerve, sometimes affecting the foot.
- Numbness in different parts of the thigh, leg, foot, and/or toes.
- Weakness while moving the thigh, knee, or foot in different directions.
- Abnormal sensations, such as a feeling of pins-and-needles and/or tingling.
It is also possible for a stabbing pain or ache to be isolated to any of these (dermatomal) areas. While lumbar radiculopathy typically affects one leg at a time, sometimes, both legs may be affected together.
An injury to the cauda equina may cause severe pain, weakness, numbness, tingling, or paralysis in both legs. There may also be a reduction or complete loss of bowel and/or bladder control. This condition, called cauda equina syndrome, is a medical emergency and requires urgent treatment to preserve leg function and restore bowel and/or bladder function.
See Cauda Equina Syndrome Symptoms
Nonsurgical treatments are often tried first for symptoms that stem from L4-L5. In rare cases, surgery may be considered.
- 1 Waldman SD. Functional Anatomy of the Lumbar Spine. In: Pain Review. Elsevier; 2009:65-66. doi:10.1016/b978-1-4160-5893-9.00029-0
- 2 Cramer GD. The Lumbar Region. In: Clinical Anatomy of the Spine, Spinal Cord, and Ans. Elsevier; 2014:246-311. doi:10.1016/b978-0-323-07954-9.00007-4
- 3 Kayalioglu G. The Spinal Nerves. In: The Spinal Cord. Elsevier; 2009:37-56. doi:10.1016/b978-0-12-374247-6.50008-0
- 4 Amin RM, Andrade NS, Neuman BJ. Lumbar Disc Herniation. Curr Rev Musculoskelet Med. 2017;10(4):507–516. doi:10.1007/s12178-017-9441-4




